PLDD – Percutaneous Laser Disc Decompression
In the procedure of percutaneous laser disc decompression, laser energy is transmitted through a thin optical fiber into the disc.
The aim of PLDD is to vaporize a small portion of the inner core. The ablation of a relatively small volume of the inner core results in an important reduction of intra-discal pressure, thus inducing a reduction of disc herniation.
PLDD is the minimally-invasive medical procedure developed by Dr. Daniel S.J. Choy in 1986 that uses a laser beam to treat back and neck pain caused by a herniated disc.
Percutaneous laser disc decompression (PLDD) is the utmost minimally invasive percutaneous laser technique in the treatment of disc hernias, cervical hernias, dorsal hernias(except for the segment T1-T5), and lumbar hernias. The procedure uses laser energy to absorb the water within the herniated nucleus pulpous creating a decompression.
The PLDD treatment is performed on an outpatient basis using only local anesthesia. During the procedure, a thin needle is inserted into the herniated disc under X-ray or CT guidance. An optical fiber is inserted through the needle and laser energy is sent through the fiber, vaporizing a tiny portion of the disc nucleus. This creates a partial vacuum which draws the herniation away from the nerve root, thereby relieving the pain. The effect usually is immediate.



The procedure appears to be nowadays a safe and valid alternative to microsurgery, with a rate of success of 80%, particularly under CT-Scan guidance, in order to visualize the nerve root and also apply energy on several points of disc herniation. This permits to have a shrinking concentrated in a bigger area, realizing minimal invasiveness on the spine to be treated, and avoiding the potential complications related to the microdiscectomy (recurrence rate of more than 8-15%, peridural scar in more than 6-10%, dural sac tear, bleeding, iatrogenic microinstability), and does not preclude traditional surgery, if needed.
Tissue Interaction with Dimed Laser
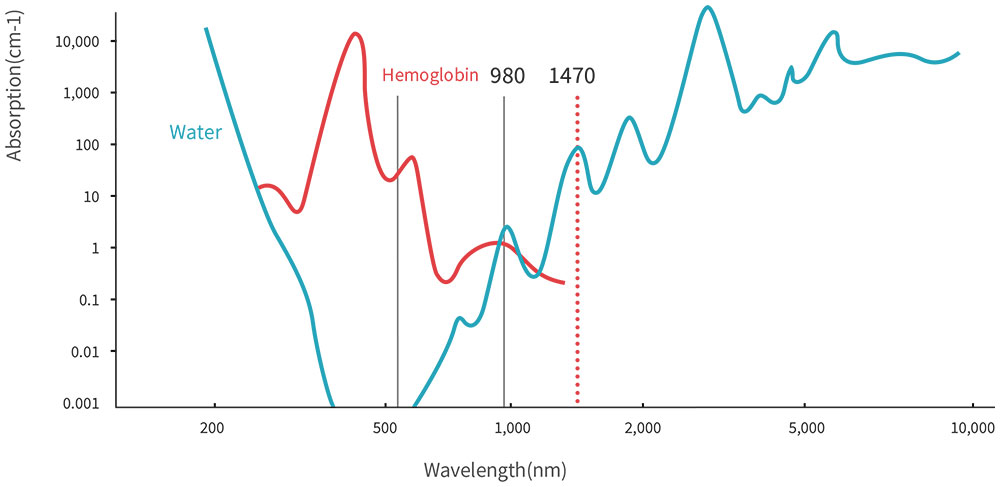
With Dimed 980nm laser, the 980nm wavelength facilitates efficient tissue ablation and coagulation by offering equal absorption by blood and water. On the other hand, with Dimed 1470nm laser, the 1470nm wavelength with higher water absorption enables precise ablation and localized heating. particularly advantageous around critical structures. its outstanding interaction with water and hemoglobin, coupled with a moderate penetration depth into disc tissue, allows safe and accurate procedures, especially in proximity to delicate anatomical structures.
Open Discectomy
This surgery will be performed under general or spinal anesthesia depending on the surgeon’s or the patient’s preferences. The patients will be positioned prone and the affected disc level is verified with fluoroscopy. A small midline incision (2–3 cm) will be made and the paravertebral muscles will be dissected unilaterally. Laminotomy will be performed when deemed necessary. In order to decompress the nerve root, the herniated disc will be removed as much as possible through a unilateral transferral approach. The wound will be closed in layers with a suction drain when necessary. Patients will be operated with loupe magnification or microscope depending on the surgeon’s preference. The participating surgeons have large experience in the technique. A standardized case record form (CRF) will register the surgeon’s findings and will be sent to the data center. Patients will be admitted to the hospital for 2–7 days depending on the usual care.
PLDD
The patient will be instructed to take a prone position on the table of the CT scan. After placing sterile drapes the level of treatment is identified by a scan. The needle entry point is anesthetized by local lidocaine injection no deeper than the facet joint. Subsequently, the 18G needle is placed centrally in the nucleus pulposus, and parallel to the endplates by means of a posterolateral approach. Through the needle, glass fiber is placed in the disc, enabling the application of laser energy (980 nm, 7 W, 0,6 s pulses, interval 1 second). After total energy of 1500 J is delivered (2000 J for levels L4-5), the PLDD procedure is finished. A control CT scan is performed to assess gas formation in the disc space. After the treatment, the patient is allowed to drink tea or coffee and is observed for 15 minutes before he/she can return home.
Full Set of Accessories
Dimed PLDD laser system is specially designed for mini-invasive surgery, providing a full set of high-quality standard and optional accessories, such as a puncture needle, Y-valve, optical fiber, safety goggles, footswitch, fiber cutter, carry case, cart, etc.
The sterile kit includes a 400-micron bare fiber with jacket protection, 2 sizes of 18G needles (length 10cm/15cm) for your choice of entry, and a Y Connector allowing for entry and suction. The connector and needles are individually packed to enable maximum flexibility in treatment.



Advantages of PLDD Laser Treatment
- It’s minimally invasive, hospitalization is unnecessary, and patients get off the table with just a small adhesive bandage and return home for 24 hours of bed rest. Then patients begin progressive ambulation, walking up to a mile. Most return to work in four to five days.
- Highly effective if correctly prescribed
- Processed under local, not general anesthesia
- Safe and fast surgical technique, No cutting, No scarring, Since only a tiny amount of disc is vaporized, there is no subsequent spinal instability. Different from open lumbar disc surgery, there is no damage to the back muscle, no bone removal, or a large skin incision.
- It’s applicable to patients who are at higher risk to open discectomies such as those with diabetes, heart disease, decreased liver, and kidney functions, etc.